A FISTULA IS A COMMUNICATION BETWEEN TWO EPITHELIAL LINED SURFACES; IN THE CASE OF ANAL FISTULAS, this communication is between the anal canal and the skin in the perianal area. Usually believed to be caused by an infected anal gland between the internal and external sphincters, the accumulation of the infected contents make their way across the sphincters and surrounding tissues, presenting at first as an abscess. This usually goes on to discharge spontaneously, causing temporary relief, but as time goes on, there may be intermittent swelling, pain and discharge, resulting in a chronic anal fistula
The key to successfully eradicating this problem hinges on the complete removal of the infected anal gland. Traditionally, this involves laying open the complete fistula tract and allowing the open wound to heal by secondary intention. While this can be performed easily with low fistula tracts, more complex tracts that traverse a higher plane involve more anal sphincter musculature and therefore need to be treated differently. Indeed, the traditional method will also damage a significant amount of anal sphincter muscle, resulting in faecal incontinence.
This incontinence will often impact the patient’s quality of life significantly, as shown by a clinical study performed in 2000 by Aguilar. In the study, patients surveyed reported that they were often more unhappy with the resulting incontinence than with the failure of the surgery in healing their fistula. It is this that prompted a change to the modern approach in the treatment of complex anal fistulas, which often focus on the preservation of anal sphincter function in addition to healing the fistula.
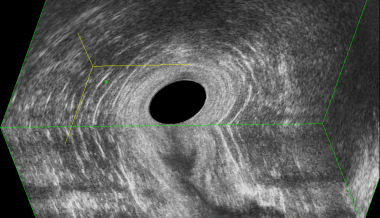
To help doctors decide when a sphincter preserving option is necessary, imaging becomes important. This can be done through endoanal ultrasonography, a convenient and accurate way to assess the fistula before the operation. When completed, 3D rendering software allows doctors to visualize and spatially orientate the fistula in relation to the anal sphincter complex. The ultrasonography is an outpatient procedure and can be performed in the clinic with minimal discomfort.
At Colorectal Clinic Associates at Mount Elizabeth Novena Hospital, we routinely employ endoanal 3D ultrasonography to image all patients presenting with or suspected to have an anal fistula or a deep-seated anal abscess. With this level of precision imaging, we are able to tailor the most appropriate surgical treatment for the patient, ensuring not only a higher degree of success but also in preserving continence.
Some of our patients come with a history of multiple failed surgeries performed elsewhere. Through imaging, we find that the most common cause of failure is in missing the source of infection i.e. not locating and removing the primary tract. |
|
The use of endoanal ultrasonography has also enabled us to determine the amount of residual functional muscle in patients who have had previous fistula surgery, allowing us to better counsel our patients on the impact of subsequent surgery on their continence.
There is also the ability to site our surgical incisions more precisely when dealing with anal fistulas. In the latest sphincter preserving approach in the treatment of anal fistulas, only a small incision is required to tackle the source of infection lying in between the inner and outer anal sphincter. Endoanal ultrasonography allows us to site the smallest incision needed in the precise location to get the job done. In this new technique (aka “LIFT” or “Ligation of Intersphincteric Fistula Tract”), patients have minimal discomfort, minimal wound care requirements and faster recovery.
With better understanding of the disease process, doctors are better able to offer minimally invasive sphincter preserving solutions. However this is only possible with the availability of precision imaging accorded by endoanal 3D ultrasonography. In contrast, traditional fistula surgery in the past was determined pretty much by what we find or what we think is the anatomy at the time of surgery. The patient would have little foreknowledge of what the surgeon will do, other than the fact that it involves painful cutting of anal sphincter muscle. Endoanal ultrasonography gives the gift of foresight to the surgeon and the patient. With a detailed roadmap, the surgeon is forewarned and in doing so, he is forearmed to cure the patient of his anal fistula.
Prof Tsang is a world renowned expert on 3D endoanal ultrasonography as well as the LIFT technique in the treatment of complex anal fistulas. He has lectured and taught extensively on this subject at numerous international meetings as faculty member and has also authored numerous papers in peer reviewed journals. Both Prof Charles Tsang and Prof Dean Koh are practising full time at Colorectal Clinic Associates at Mount Elizabeth Novena Hospital and are Adjunct Associate Professors of Surgery at the Yong Loo Lin School of Medicine, National University of Singapore.
|